Discussion
Discussion
Causes of Alagille syndrome
Last updated Dec. 17, 2024, by Marisa Wexler, MS
 Fact-checked by Marta Figueiredo, PhD
Fact-checked by Marta Figueiredo, PhD
Alagille syndrome is a rare genetic disorder caused by mutations in genes of the Notch signaling pathway, which is involved in embryonic development. Disruptions in this pathway lead to abnormalities and errors during early development that ultimately give rise to the symptoms of Alagille syndrome.
The disease most commonly affects the liver, particularly the development of bile ducts, the tubes that carry the digestive fluid bile from the liver to the intestines. When bile ducts are fewer than normal, bile flow becomes disrupted, which can cause liver damage and reduce the absorption of fat-soluble vitamins.
Besides liver disease, Alagille can cause other issues, including heart defects or heart murmur, characteristic facial features including deep-set eyes, abnormal spinal bones named butterfly vertebrae, and posterior embryotoxon, or an abnormal white ring in the membrane that covers the eyeball.
Because signs and symptoms of the disease can vary widely among patients and overlap with other conditions, it can be difficult to reach a diagnosis of Alagille syndrome. Identifying Alagille-causing mutations is a key part of obtaining an accurate diagnosis to ensure patients receive timely and appropriate disease treatment, which can range from a liver transplant to nutritional support or medications to ease symptoms.
Knowing which mutations a person has also can help to predict the risk of passing the disease to future generations.
Genetic causes of Alagille syndrome
Alagille syndrome is caused by gene mutations that are present from the earliest stages of embryonic development. Variations in two genes, JAG1 and NOTCH2, are the only definitively established causes of Alagille syndrome. These genes code for a ligand and a receptor that interact with each other to activate the Notch signaling cascade.
Notch is a major signaling pathway that regulates cell fate during embryonic development and adult life. Mutations in Notch genes are known to cause developmental abnormalities in the liver, blood vessels, heart, skeleton, face, eyes, and kidneys.
Issues with the JAG1 gene
Mutations in the JAG1 gene are by far the most common Alagille syndrome cause, reported in about 94% of all cases.
JAG1 provides instructions to make a protein called Jagged-1 (JAG1) that sits on the surface of cells. It works as a ligand that interacts with Notch receptor proteins, including NOTCH2, that are located at the surface of a neighboring cell, which activates the Notch pathway on that cell.
The majority of JAG1-related Alagille syndrome cases are caused by protein-truncating mutations (75%), meaning they result in a shorter JAG1 protein that cannot function properly. Some cases of Alagille syndrome also are caused by whole gene deletions or other major mutations that result in no protein being produced.
Less frequently, Alagille patients carry JAG1 missense mutations, where a single letter change in the DNA sequence can result in the substitution of one amino acid (the protein’s building blocks) for another in the protein that is produced. Depending on the importance of the affected amino acid and its role in the protein, this change can alter JAG1’s structure or function.
In either case, the end result is that Notch signaling is disrupted, ultimately driving abnormalities in development. Notably, the JAG1-NOTCH2 interaction is essential for the development of bile ducts, so a reduced number of bile ducts in the liver is a hallmark feature of Alagille.
JAG1 also is essential to regulating the development of blood vessels, including those of the coronary arteries that supply blood to the heart muscle and of the pulmonary arteries that transport blood from the heart to the lungs. It also has been reported to have a role in the development of the eyes, bones, and kidneys. As a result, these organs and tissues are commonly affected in Alagille.
Issues with the NOTCH2 gene
Mutations in the NOTCH2 gene, which provides instructions to make a protein of the same name, account for about 2.5% of all Alagille cases.
Like JAG1, the NOTCH2 receptor protein is found at the surface of cells, but it works like a signaling receiver instead of a signaling sender. It is known to be involved in several developmental processes that are affected in Alagille syndrome.
Contrary to what is observed for JAG1, most Alagille-causing NOTCH2 mutations are missense (68%). This suggests that more severe mutations, which entirely abrogate the protein’s function, may not be compatible with fetal development and result in a spontaneous pregnancy termination. Available evidence so far suggests that NOTCH2 variants result in a protein that cannot be adequately activated by JAG1.
NOTCH2 mutations seem to result in a lower frequency of heart involvement, bone abnormalities, and facial features compared with JAG1 mutations. These differences help to shed light on those organs whose development mainly rely on JAG1-NOTCH2 signaling, and those that mainly dependent on other JAG1-related mechanisms.
No known issues with the JAG1/NOTCH2 genes
Although mutations in JAG1 and NOTCH2 are the only established causes of Alagille, there are cases in which patients exhibit typical signs of the disease but test negative for mutations in those two genes. It remains unclear whether this is due to limitations of conventional genetic testing, the presence of a different disease with overlapping Alagille features, or the existence of mutations in other genes that may act as Alagille syndrome causes. Comprehensive genetic tests may help clarify these cases.
Inheritance pattern and de novo mutations
In many cases, Alagille-causing mutations are inherited from a biological parent with Alagille syndrome. But the same mutation can result in very different disease manifestations, meaning that a person without any notable Alagille signs or symptoms can have a child with severe disease.
Still, Alagille syndrome is more commonly associated with de novo mutations, which are not inherited from parents and instead occur spontaneously when the DNA is copied during cell division.
Inheritance pattern of Alagille syndrome
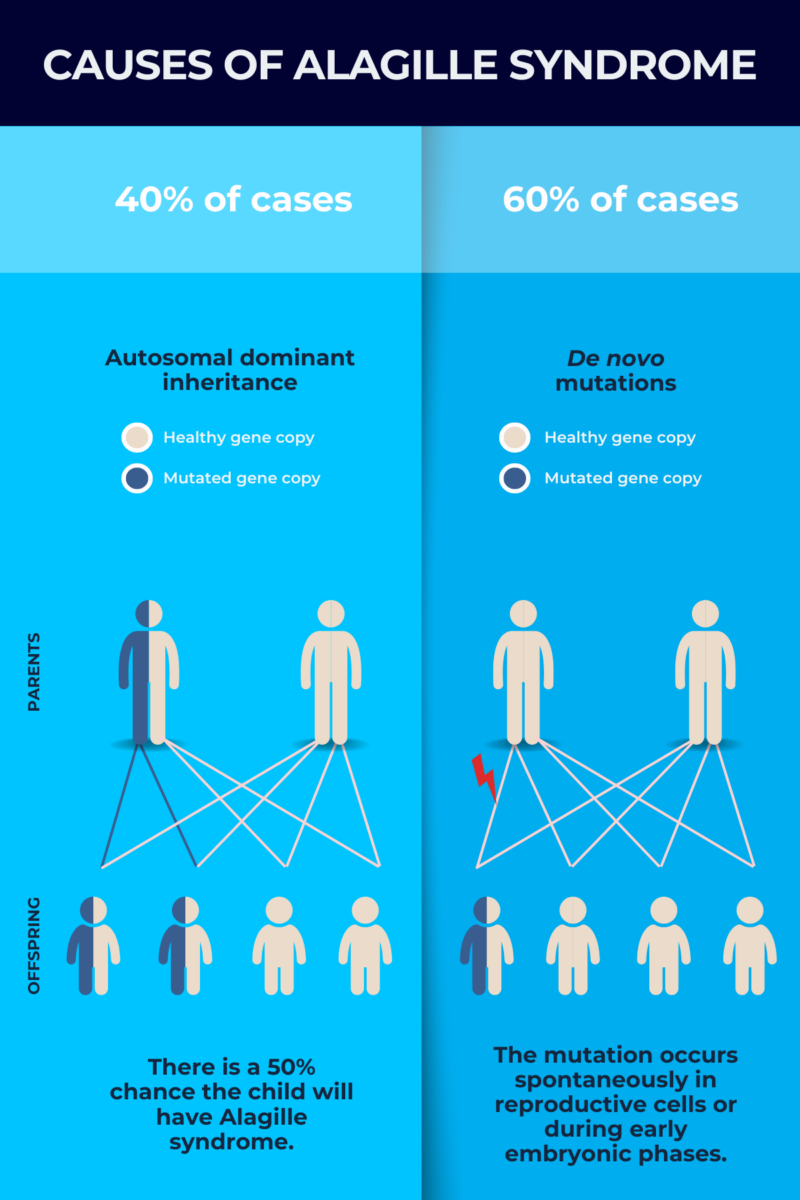
About 40% of children with Alagille syndrome inherit their disease-causing mutation from a parent.
As happens with most genes, everyone has two copies of JAG1 and NOTCH2, one from each biological parent. Alagille syndrome inheritance occurs in an autosomal dominant pattern, meaning that one mutated copy of either gene is sufficient to cause the disease.
If a person with Alagille syndrome reproduces, there’s a 50% chance that the child will inherit the mutation and develop the disease. Thus, adults with Alagille who are considering having children may choose to undergo preimplantation genetic testing, where assistive reproductive techniques such as in vitro fertilization or IVF are used to conceive, and the embryo is first tested for Alagille before being implanted into the uterus to commence pregnancy.
It is possible to perform genetic testing during pregnancy to see if a baby will carry the mutation.
If a child with Alagille syndrome is born to people who aren’t themselves diagnosed with the condition, it’s often recommended that the parents undergo testing to see if either of them carries a disease-causing mutation, even if neither has any obvious disease signs. If no mutation is detected, Alagille likely arose due to de novo mutations.
De novo mutations
In the roughly 60% of cases where Alagille syndrome is not inherited, the disease is associated with de novo mutations that spontaneously develop in sperm, egg cells, or during the early embryonic phases.
In these cases, even though neither parent carries a disease-causing mutation, genetic testing can be done on their sperm or egg cells to provide information about the risk of Alagille syndrome in future children. Talking to a specialist like a genetic counselor can help in understanding the results of genetic testing.
Other factors
Alagille equally affects people of different sexes, races, ethnicities, and geographic regions, but the type and severity of symptoms can vary greatly, even within families — and between twins — with the same disease-causing mutation.
While this suggests that environmental factors may contribute to Alagille’s clinical profile, the exact factors have yet to be established. Another possible explanation is the existence of genetic modifiers, or genes whose variations do not directly cause Alagille but modify the effects of JAG1 and NOTCH2 mutations. Several potential modifiers that may help to explain the variability in Alagille symptoms have been identified.
Environmental factors also may contribute to the development of de novo mutations that cause Alagille. While some of these mutations occur by chance during cell division, de novo mutations can arise as a result of paternal or maternal exposure to environmental factors, such as radiation and polycyclic aromatic hydrocarbons, a class of chemicals that form during incomplete burning of coal, oil, and gas. More studies are needed to determine the contribution of environmental factors to the development of Alagille-causing mutations.
Liver Disease News is strictly a news and information website about the disease. It does not provide medical advice, diagnosis or treatment. This content is not intended to be a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition. Never disregard professional medical advice or delay in seeking it because of something you have read on this website.
Related articles
-
Discussion
-

-
 Discussion
Discussion
-
-

-