 Discussion
Discussion
Alagille syndrome symptoms
Last updated Oct. 16, 2024, by Marta Figueiredo, PhD
 Fact-checked by Inês Martins, PhD
Fact-checked by Inês Martins, PhD
Alagille syndrome is a rare genetic disease that can cause a wide variety of symptoms. The most common Alagille syndrome symptoms are liver problems that arise due to abnormalities in the bile ducts, which carry the digestive fluid bile from the liver to the intestines. However, abnormalities in the heart, face, eyes, kidneys, bones, and blood vessels are also common in people with the condition.
The disease is caused by defects in embryonic development due to mutations in one of two genes — JAG1 or NOTCH2 — belonging to a key signaling pathway called Notch that’s involved in early development processes.
The type and severity of Alagille syndrome symptoms can vary widely from person to person, even within families sharing the same disease-causing mutation. Some patients may have no to very subtle Alagille syndrome signs that can go unnoticed, while others may develop life-threatening complications.
Achieving an Alagille syndrome diagnosis and initiating treatment early on is essential to prevent the more serious consequences of the disease, particularly those associated with liver and heart problems.
Common symptoms of Alagille syndrome
Alagille syndrome signs, particularly those related to liver problems, usually manifest during infancy or early childhood, but milder cases can be detected only later in life, during adulthood.
The most common symptoms of Alagille include:
- liver problems
- heart defects
- characteristic facial features
- eye abnormalities.
Liver symptoms
Liver problems are typically the first notable sign of Alagille, often presenting in the first three months of life and affecting 89%-100% of cases. Liver problems in Alagille syndrome are most commonly caused by intrahepatic bile duct paucity, or a lower number of bile ducts inside the liver, although other bile duct abnormalities also may be the cause.
These bile duct problems can slow or stall the flow of bile, a condition called cholestasis. Bile is a digestive fluid that’s essential for the digestion and absorption of dietary fats and vitamins. It also carries certain waste products, such as excess cholesterol, toxins, and bilirubin, a yellow-reddish compound that’s produced when red blood cells are broken down, into the intestines to be excreted in stools.
However, in people with Alagille, cholestasis causes bile to accumulate inside the liver, damaging the organ. Certain bile compounds and waste products that are not being properly eliminated in feces will also leak into the bloodstream. Together, these abnormalities result in a number of liver problems in Alagille syndrome, including:
- jaundice, a yellowing of the skin and whites of the eyes caused by excess bilirubin in the bloodstream
- itchy skin, or pruritus, associated with the buildup of bile acids and other bile components in the blood
- dark urine and pale stools, due to excess bilirubin in the blood that is excreted through urine instead of feces, making the former look darker than usual and the latter lighter than normal
- loose and foul-smelling stools, due to their high fat content
- xanthomas, or raised skin lesions that appear waxy and yellowish, that consist of cholesterol deposits underneath the skin
- failure to thrive, weak bones, or easy bleeding due to problems with absorbing fat-soluble vitamins such as vitamins A, D, E, and K
- enlarged liver or spleen, detected through medical examination.
Heart symptoms
Congenital heart problems, or those present at birth, are a common Alagille syndrome symptom, affecting more than 90% of patients.
Heart defects in Alagille syndrome most commonly include peripheral pulmonary stenosis, in which the pulmonary arteries that carry blood from the heart to the lungs are narrowed, making it harder for the heart to pump out blood. This structural abnormality, reported in about two-thirds of Alagille patients, can be first detected by the presence of a heart murmur, or an extra, unusual sound during a heartbeat.
A complex heart defect called tetralogy of Fallot is also reported in up to 16% of cases. It consists of a combination of four co-occurring abnormalities:
- pulmonary artery stenosis
- ventricular septal defect, or a hole between the right and left ventricles (the lower heart chambers)
- abnormal enlargement of the right ventricle
- an abnormal positioning of the aorta, the body’s largest vessel, that causes it to receive blood from both ventricles instead of just the left ventricle.
Tetralogy of Fallot can limit the amount of oxygen in the blood, resulting in cyanosis, a bluish discoloration of the skin.
Less common heart defects in Alagille syndrome include:
- ventricular septal defect alone
- atrial septal defect, or a hole between the upper heart chambers (right and left atria)
- aortic stenosis, which occurs when the valve between the left ventricle and the aorta is narrowed and does not open fully, limiting blood flow
- coarctation of the aorta, or a narrowing of a section of the aorta that also impairs blood flow.
Facial symptoms
Up to 95% of Alagille patients show characteristic facial features, including a broad forehead, deeply set and widely spaced eyes, a straight nose with a bulbous tip, and a pointed chin. These facial features of Alagille syndrome, which can make the face look like an inverted triangle with the tip pointing down, may not be as easy to detect in infants.
Alagille patients may also present other changes in the jaw, teeth, and gums. As patients get older, the lower jaw and chin may appear larger and more prominent, a condition called mandibular prognathia.
Eye symptoms
Eye problems have been reported in more than 90% of Alagille patients. The most common eye abnormality, estimated to affect more than three-quarters of patients, is posterior embryotoxon, which is marked by a white ring lining the cornea — the thin, transparent membrane that covers the eyeballs.
This condition, detected only via an eye exam, is also present in up to 15% of the general population. While it does not typically affect vision, it can be a useful diagnostic marker of Alagille.
Another common eye manifestation is optic disk drusen, which refers to deposits of fatty proteins and calcium in a region at the back of the eyes. This abnormality, which is also detected through specialized eye exams, impacts about 90% of all Alagille patients compared with about 2% of the general population.
People with Alagille may also present with other eye abnormalities and symptoms, including:
- pigmentary retinopathy, or progressive degeneration of the retina (the innermost, light-sensitive layer of tissue of the eye) that is marked by pigment deposition
- changes in the macula, the central part of the retina
- abnormalities in the iris, the front, colored part of the eye
- problems with peripheral, or side, vision
- night blindness
- sensitivity to light
- progressive loss of vision.
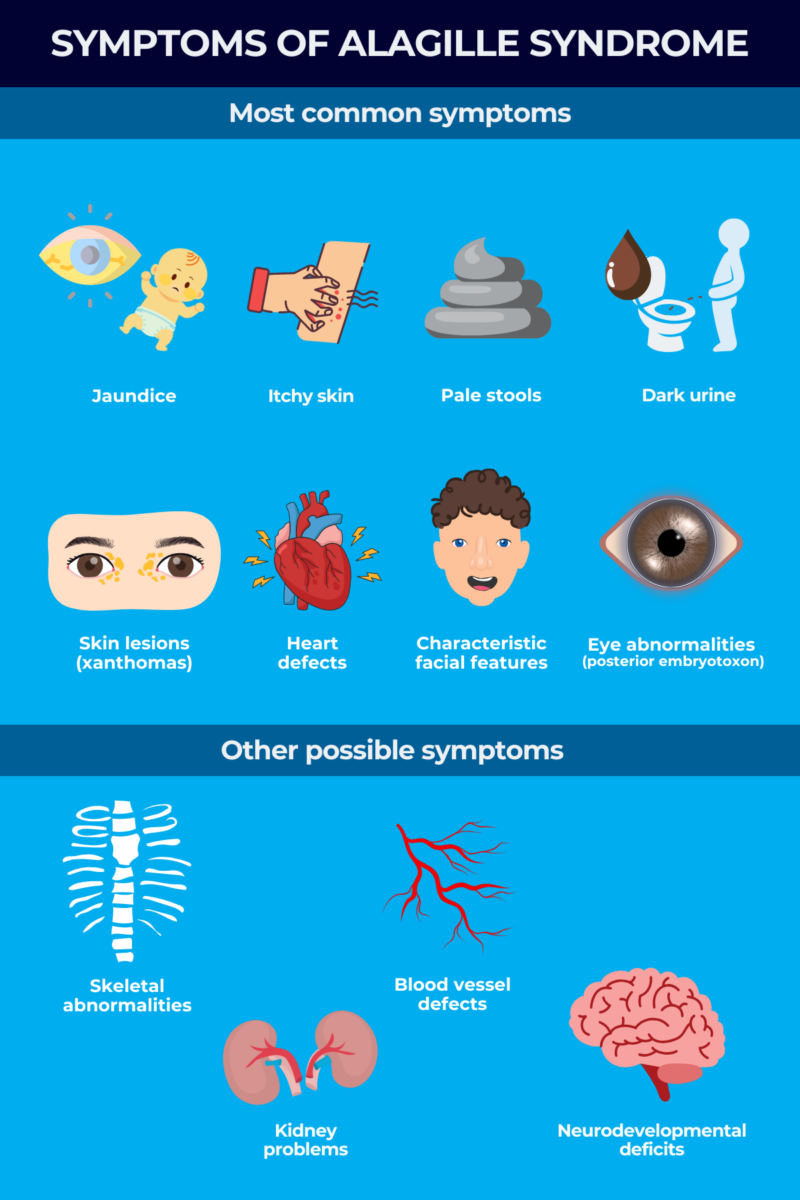
Other possible symptoms
People with Alagille syndrome can also present a range of other symptoms, including:
- skeletal abnormalities
- kidney problems
- blood vessel, or vascular, abnormalities
- neurodevelopmental deficits.
Skeletal abnormalities, reported in 33% to 93% of Alagille patients, may include:
- butterfly vertebra, the most common bone abnormality in Alagille, which is marked by an irregular, butterfly-like shape of the vertebrae (the bones that make up the spine)
- hemivertebrae, where half of a vertebrae does not form
- fusion of adjacent vertebrae
- spina bifida occulta, where there is a gap between vertebrae
- craniosynostosis, a condition in which the bones in a baby’s skull fuse too early
- additional creases in fingers and toes and shorter bones at the end of fingers
- abnormalities in the bones in or around the ear, which can raise the risk of chronic ear infection and hearing loss
- increased risk of bone fractures, likely due to intrinsic skeletal defects and cholestasis-related nutritional deficiencies.
Kidney defects, present in more than one-third of Alagille patients, can include:
- abnormally small or underdeveloped kidneys
- renal tubular acidosis, when the kidneys fail to properly remove acids from the blood into the urine and acids accumulate in the blood
- a blockage in the region where the kidneys connect to the ureters (the tubes that carry urine to the bladder), impairing urine flow and causing kidney swelling and damage
- cysts, or small pockets of tissue that may be filled with fluid.
Kidney problems may be more common in people carrying mutations in the NOTCH2 gene, which are estimated to make up about 2% of all patients.
Abnormalities in blood vessels other than those in the heart, including in the brain, liver, lungs, and kidneys, also may affect about one-third of Alagille patients. These may include:
- brain aneurysm, or a bulging, weakened area in a blood vessel in or around the brain, which can increase risk of bleeding-related stroke
- moyamoya syndrome, a progressive disorder marked by the narrowing or blocking of the carotid artery, the major artery that delivers blood to the brain, which can lead to stroke related to reduced blood flow
- structural abnormalities, including elongation and narrowing, of blood vessels in the neck, liver, kidneys, and abdomen.
Children with Alagille syndrome may exhibit neurodevelopmental delays, which seem to occur more commonly than in people with other inherited cholestatic liver diseases. Some studies report the need for special education in about half of Alagille cases.
In addition, some patients may also experience slower motor development, delayed puberty, high-pitched voice, and functional problems in the pancreas, an organ that normally helps make enzymes that aid in digestion.
Early signs to look out for
Because Alagille syndrome symptoms can vary widely between patients, identifying Alagille syndrome isn’t always easy. A diagnosis can be further complicated by the presence of subtle signs that may not necessarily be specific to the disease.
The sooner doctors confirm a diagnosis, the earlier they can establish an appropriate Alagille syndrome treatment plan. This may involve medications and surgical procedures to manage disease symptoms, avoid potential life-threatening complications, and improve life quality.
Some of the earliest Alagille syndrome symptoms, often noticeable in the first few months of life, may include:
- jaundice
- elevated markers of liver damage in the blood
- pale, loose stools
- dark urine
- poor growth or weight gain.
Later, during early childhood, Alagille symptoms may include:
- persistent jaundice
- severe itching
- xanthomas
- facial features of Alagille syndrome.
If parents or caregivers detect these signs and symptoms, they should discuss them with a healthcare provider, who can assess children for other Alagille syndrome signs, including heart murmur, butterfly vertebrae, and posterior embryotoxon.
Severe complications
When left unnoticed and untreated, certain Alagille syndrome symptoms can increase the risk of serious complications. In about 15% of Alagille cases, persistent cholestasis and progressive liver disease lead to irreversible liver scarring, or cirrhosis, and liver failure, which can be life-threatening and may require a liver transplant.
Portal hypertension, or increased pressure in the vein that transports blood from the gastrointestinal system to the liver, is also common among older patients. This complication can lead to an enlarged liver or spleen, spider veins (red, spider-like blood vessels under the skin), swollen veins in the esophagus or abdomen, and fluid buildup in the abdomen.
People with Alagille are also at an increased risk of hepatocellular carcinoma, the most common type of liver cancer.
In addition to severe liver disease, complex congenital heart diseases like tetralogy of Fallot and other vascular anomalies such as brain bleeding can also contribute to early death in Alagille patients. Evidence suggests that those with both severe liver and heart disease at birth show the poorest survival.
While Alagille syndrome signs may range in severity from almost unnoticeable to life-threatening, certain symptoms may indicate more severe disease that may need more urgent medical attention, including:
- severe cholestasis and its associated signs, including jaundice, intense itching, dark urine, and pale stools
- serious heart defects, such as tetralogy of Fallot, that may affect breathing and cause cyanosis
- severe failure to thrive
- vascular problems
- kidney disease
- multiple organs significantly affected by the disease.
While some of these signs and symptoms can only be detected with specific medical exams, others may be easily noticed by parents or caregivers, who should immediately reach out to healthcare providers to discuss next steps.
Liver Disease News is strictly a news and information website about the disease. It does not provide medical advice, diagnosis or treatment. This content is not intended to be a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition. Never disregard professional medical advice or delay in seeking it because of something you have read on this website.
Related articles
-
Discussion
-
-

-
 Discussion
Discussion
-
-
