Biliary atresia diagnosis
Last updated Jan. 15, 2025, by Lindsey Shapiro, PhD
 Fact-checked by Marta Figueiredo, PhD
Fact-checked by Marta Figueiredo, PhD
Reaching a diagnosis of biliary atresia, a rare liver disease affecting infants in which bile ducts inside and/or outside the liver are blocked or absent, involves a series of different tests.
Bile ducts are a series of tubes that carry the digestive fluid bile from the liver, where it is made, to the gallbladder, where it is stored, and then to the small intestine, where it’s used to aid in digestion. When there are problems with these ducts, the flow of bile is stalled — a condition called cholestasis — and bile toxically accumulates in the liver and damages it.
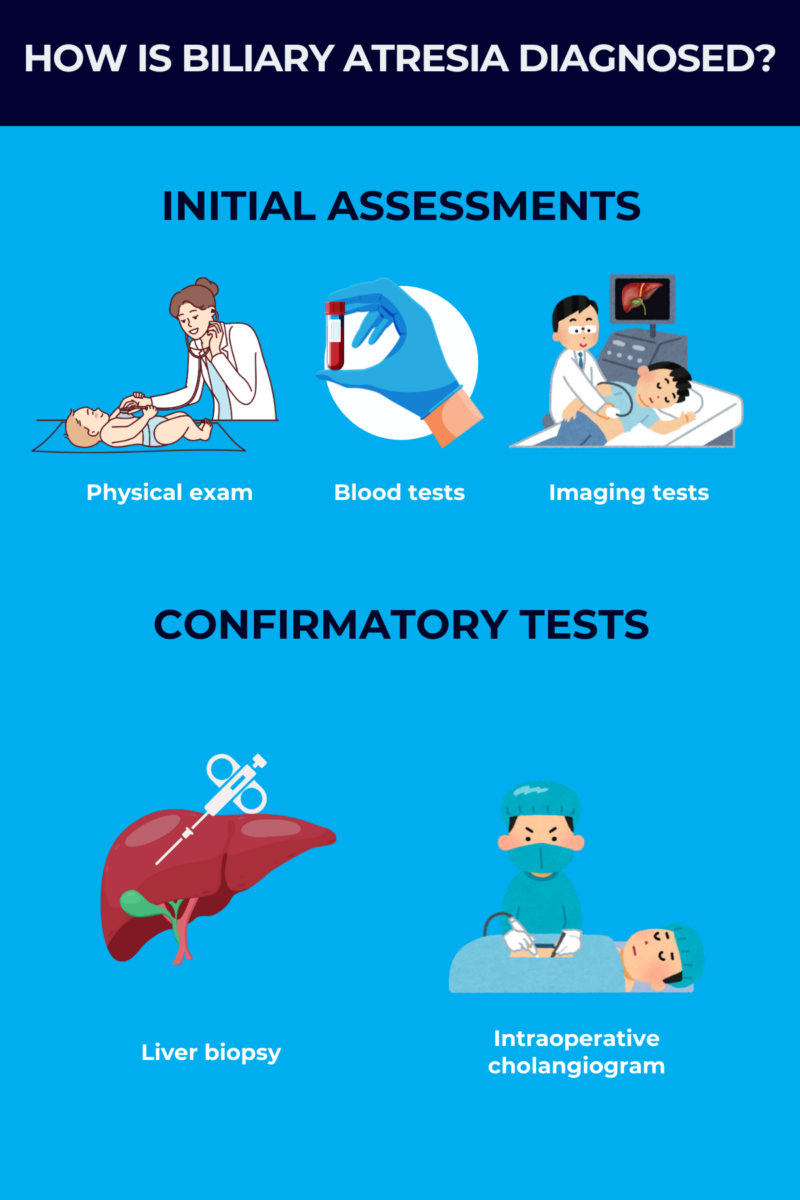
A diagnosis of biliary atresia may include physical exams, blood or urine tests, imaging studies, and liver biopsies, which together can point toward biliary atresia and rule out other diseases.
The gold standard test to diagnose the disease is a surgical procedure called a cholangiogram. If the results are positive, a definite diagnosis can be made, and the surgeon will often immediately initiate surgical treatment for the disease.
The standard surgery for biliary atresia, known as the Kasai procedure, can substantially improve outcomes, particularly when done at a very young age and before significant liver damage occurs. An early and accurate diagnosis is critical for children with biliary atresia to have the best possible outcomes. An early diagnosis will also help to avoid or delay more serious consequences, such as the need for a liver transplant.
Initial steps for diagnosing biliary atresia
There’s no way to predict ahead of time whether a baby will have the condition, so the process of figuring out how to diagnose biliary atresia often starts when an infant shows signs of liver disease.
Doctors will generally start by performing a physical exam and collecting a medical history. While biliary atresia does not run in families, other conditions with overlapping symptoms might, so a doctor may also ask if there’s a family history of related symptoms. If biliary atresia is suspected, a series of other tests may be performed to look at how the liver is functioning and to check for blocked bile ducts.
Symptoms that prompt diagnosis
The earliest symptoms of biliary atresia in infants include:
- jaundice, or yellowing of the skin and whites of the eyes
- dark urine
- pale stools that may be clay-colored, gray, or white, also called acholic stools.
These biliary atresia clinical manifestations result from the abnormal accumulation of bilirubin, a yellow-reddish waste product that’s normally incorporated into bile to be excreted in feces, in the bloodstream.
In the most common type of biliary atresia, called perinatal biliary atresia, babies may appear healthy at birth, but symptoms will develop over the first few weeks of life. A smaller proportion of patients — about 10%-20% — have fetal biliary atresia, in which symptoms are evident immediately at birth and are sometimes accompanied by problems in other organs.
If parents or caregivers notice symptoms of biliary atresia in their baby, they should contact a healthcare provider for further medical evaluation.
Temporary newborn jaundice is seen in many healthy babies in the first week or two of life. But if jaundice persists beyond the first two weeks after birth, babies should be evaluated for biliary atresia or other liver conditions.
Physical examination
The first step toward reaching a biliary atresia diagnosis when a baby has symptoms is a physical exam. During that visit, a doctor will:
- look for signs of jaundice
- feel the baby’s abdomen to check for an enlarged liver or spleen
- check the color of the baby’s urine and stools
- examine the baby’s body for other birth defects that may happen in biliary atresia.
Blood tests
A healthcare provider may also order blood tests to look for indicators of biliary atresia. These tests can also help rule out other liver diseases that may have similar symptoms.
Doctors will likely look at levels of bilirubin and related molecules in the blood. Total blood bilirubin levels are elevated in biliary atresia because the bilirubin is not being properly transported to the intestines for excretion.
Bilirubin tests can also help doctors understand the type of jaundice a baby has. Biliary atresia is characterized by obstructive jaundice (post-hepatic jaundice) when the flow of bile out of the liver is blocked. This is accompanied by an increase in a form of bilirubin that’s already been processed by the liver to be incorporated into bile, called conjugated (direct) bilirubin.
Other things doctors may check for in blood tests include:
- levels of gamma-glutamyl transpeptidase, a liver enzyme that’s elevated in the blood when bile ducts are blocked
- levels of other enzymes and proteins made by the liver
- blood clotting, as many clotting players are produced by the liver or absorbed in the intestines through the action of bile
- antibodies against specific microbes, including Toxoplasma gondii and herpes simplex virus, which can be another cause of enlarged liver in newborns
- levels of alpha-1 antitrypsin, which can rule out an overlapping condition called alpha-1 antitrypsin deficiency that causes cholestasis.
Imaging tests for biliary atresia
Imaging tests might also be used to visualize the liver and surrounding bile ducts to identify any abnormalities consistent with biliary atresia. These include:
- abdominal ultrasound
- hepatobiliary iminodiacetic acid (HIDA) scan.
An abdominal ultrasound uses sound waves to create images of organs, including the liver and gallbladder. In babies with biliary atresia, the gallbladder is often absent, small, or shrunken on an ultrasound. Another biliary atresia-related finding on ultrasound is the triangular cord sign, a triangular cord of fibrous tissue that’s thought to be a remnant of a bile duct outside the liver. An ultrasound can also help rule out other causes of cholestasis.
A Hida scan for biliary atresia, also known as cholescintigraphy or hepatobiliary scintigraphy, is used to track bile flow from the liver to the gallbladder and the intestines. With this test, a small amount of a radioactive tracer is injected into a vein in the arm, which will be taken up by bile-producing liver cells. A specialized scanner is then used to visualize the tracer and take pictures of it as it moves through the body, helping to track bile flow. In babies with biliary atresia, the flow of bile into the intestines is blocked, so the tracer won’t be detected there.
Confirmatory testing
When noninvasive tests suggest the presence of biliary atresia, a doctor may perform some more invasive tests to help confirm the diagnosis.
A liver biopsy — in which a small sample of liver tissue is collected and analyzed in the lab — can help doctors diagnose biliary atresia and rule out other liver problems. It usually involves inserting a hollow needle through the abdomen and into the liver to collect a liver sample. Some liver biopsy features that suggest biliary atresia include bile accumulation (bile plugs), infiltration of inflammatory cells, tissue scarring, and ductular reaction, or a response to liver injury where bile duct cells grow excessively.
While other tests can help point doctors toward biliary atresia, the most accurate way to definitively confirm a biliary atresia diagnosis is through an explorative surgical procedure called an intraoperative cholangiogram. In this procedure, a special dye is injected into the bile ducts and gallbladder through a small, surgical cut in the abdomen while the infant is under anesthesia. An X-ray is then used to visualize the movement of the dye and create detailed images of the bile ducts. If the dye fails to move through the bile ducts — reflecting absent or blocked ducts — a biliary atresia diagnosis can be confirmed.
If biliary atresia is confirmed during cholangiopathy, doctors will typically immediately perform the Kasai procedure, which creates a new path for bile to flow from the liver into the intestines. The cholangiogram is usually performed last, after less invasive tests are done and indicate that biliary atresia is likely.
Differential diagnosis of biliary atresia
There are a number of other pediatric diseases marked by cholestasis that can cause overlapping symptoms with biliary atresia. As these conditions require different management strategies, it’s important to rule them out before making a definitive diagnosis of biliary atresia and initiating treatment.
Some conditions that might be considered in the differential diagnosis of biliary atresia include:
- neonatal hepatitis
- Alagille syndrome
- progressive familiar intrahepatic cholestasis
- alpha-1 antitrypsin deficiency
- Caroli disease
- bile duct cysts
- disorders marked by problems in the metabolism of fatty molecules
- infections that can be passed from the mother to the baby during pregnancy or birth, such as those caused by Toxoplasma gondii, rubella virus, cytomegalovirus, or herpes simplex virus.
Doctors can usually distinguish biliary atresia from these other causes of infant cholestasis through a series of diagnostic tests, including blood tests, imaging scans, and liver biopsies.
Challenges in diagnosing biliary atresia
As with any rare disease, it can be challenging to accurately establish a biliary atresia diagnosis, especially because the earliest symptoms, such as jaundice and stool changes, are nonspecific and can overlap substantially with other causes of cholestasis in newborns.
Also, because the initial noninvasive tests, such as blood tests and ultrasounds, aren’t usually enough to definitively diagnose the disease on their own, the diagnostic process can be long.
Pediatricians and other primary care providers might not be familiar with how to diagnose biliary atresia or recognize the signs of the rare disease. If a baby is experiencing signs of biliary atresia or other liver conditions, it is important for families to seek referrals to specialists with the expertise necessary to definitively diagnose and treat it as promptly as possible.
Next steps after a biliary atresia diagnosis
After an infant is diagnosed with biliary atresia, it’s critical for treatment to be initiated right away. Impaired bile flow can quickly lead to serious complications, such as irreversible liver scarring (cirrhosis), portal hypertension (increased pressure in the liver’s main blood vessel), or liver failure that requires a liver transplant.
The diagnosing doctor may refer families to specialists such as hepatologists, who focus on liver diseases, or gastroenterologists. These specialists may help plan for the next steps in a child’s treatment plan.
When possible, the Kasai procedure should be performed immediately after a biliary atresia diagnosis, as this will provide the best possible outcomes for the child. However, the procedure is not a cure for biliary atresia, so families will need to work with healthcare providers to develop a care plan for ongoing management and follow-up, even after surgery.
This may include supportive care medications, nutritional support such as high-calorie liquid feedings, or other lifestyle changes that can help patients stay as healthy as possible in the long term.
Liver Disease News is strictly a news and information website about the disease. It does not provide medical advice, diagnosis or treatment. This content is not intended to be a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition. Never disregard professional medical advice or delay in seeking it because of something you have read on this website.
Related articles
-
-
 Discussion
Discussion
-
-
 Discussion
Discussion
-

-